ICU Chest Films > X-Ray Technique
X-Ray Technique
![]()
The appearance of the chest radiograph is affected by the AP positioning, supine positioning, and the degree of inspiration. Note the differences between the AP and PA chest exams below.
The AP view results in the magnification of anterior structures such as the clavicle, sternum, and heart, that can often be significant. There can be up to a 15% difference between the width of the mediastinum in a 72-inch PA and a 40-inch AP view. Furthermore, on an AP view the medial border of the scapula is projected several centimeters further into the lung.
Supine positioning also widens the mediastinum and heart due to gravitational effects. In addition, supine positioning changes the physiology of the pulmonary vasculature, putting more flow to the upper lobes and making diagnosis of cephalization (see fluid section) more difficult. Supine films also often make differentiating between pleural effusion and parenchymal processes difficult, and may make detecting a pneumothorax difficult or impossible.
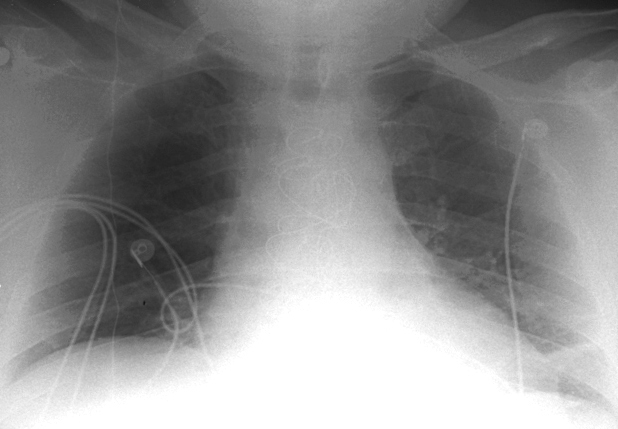
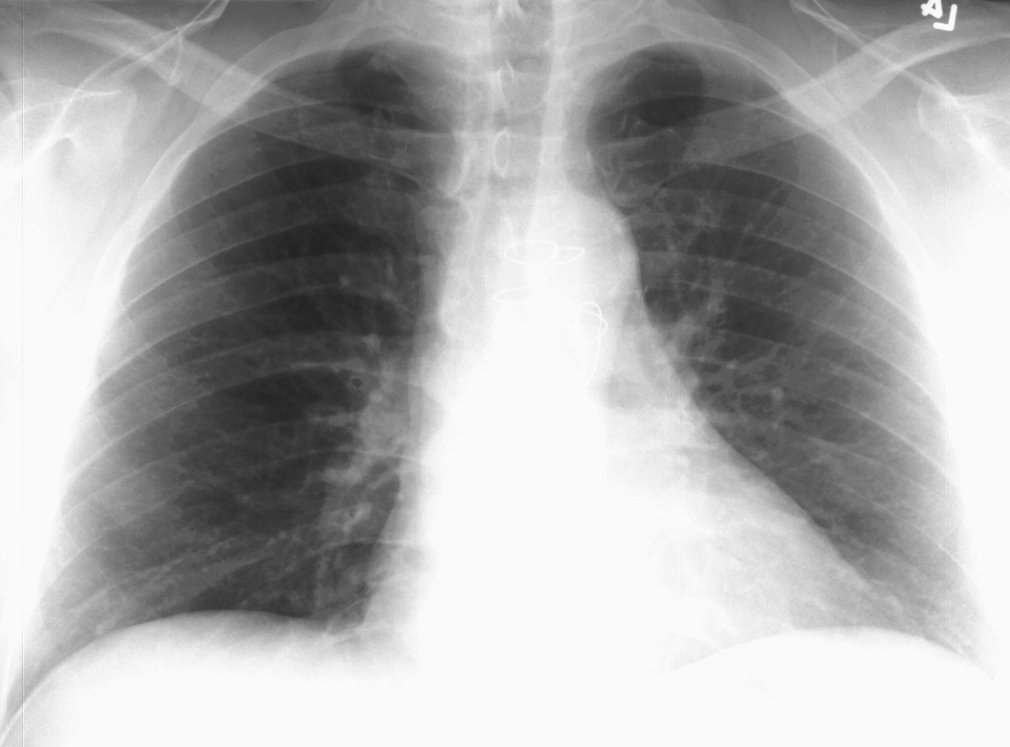
Anteroposterior (AP) and Posteroanterior (PA) views of a normal chest,
respectively.
Ideally, the radiograph should be taken at the peak of inspiration. This often presents a challenge in patients who are uncooperative or are suffering from post-operative pain. Incomplete inspiration can make evaluation problematic and diagnoses such as basilar atelectasis and lung edema more difficult. Also, incomplete inspiration may cause significant changes in the apparent size of the heart and mediastinum. The diameter of a patient's mediastinum may differ by up to 50% between an expiratory supine AP and a erect inspiratory PA.
Despite the decreased sensitivity and specificity of ICU chest films they are the most commonly ordered radiologic examination for inpatients. Their use stems from the fact that studies have shown that up to 65% of ICU chest films may reveal a significant or unsuspected process. Currently, the American College of Radiology (ACR) suggests that daily chest radiographs be obtained on patients with acute cardiopulmonary problems and those receiving mechanical ventilation. Otherwise, only initial chest radiographs are needed for the placement or change of indwelling lines or devices.
![]()
![]()
© Copyright Rector and Visitors of the University of Virginia 2013