ICU Chest Films > Fluid in the Chest > Pleural Effusions > Subpulmonic Effusions and Interlobar Pleural Effusions
Subpulmonic Effusions and Interlobar Pleural Effusions
![]()
Subpulmonic effusions are a frequent occurrence in the ICU patient. Up to a liter of fluid may collect between the diaphragm and the lung without blunting of the costophrenic angle. Radiographically, subpulmonic effusions appear as a raised diaphragm with flattening and lateral displacement of the dome. The gastric bubble and splenic flexture of the colon show displacement inferiorly. The distance between the lung and the stomach bubble will exceed 2 cm in subpulmonary effusions. The lateral decubitus film can usually resolve any question of the presence of a subpulmonary effusion.
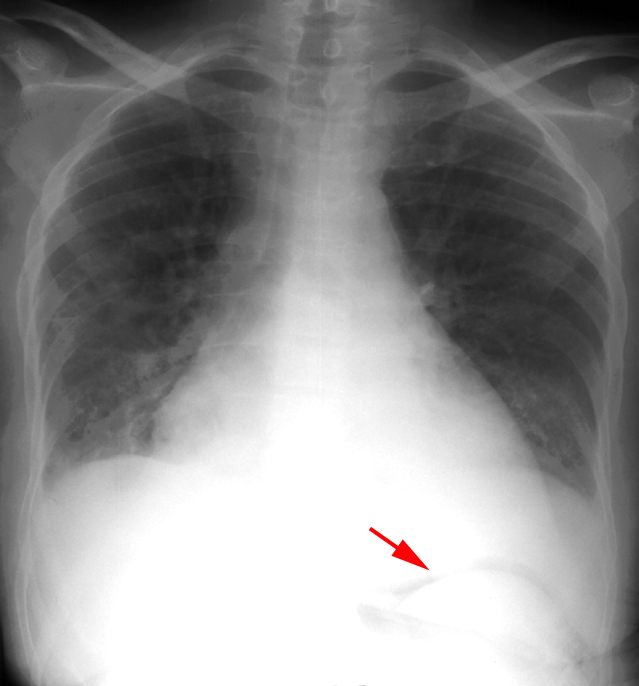
This is a sitting AP film of a patient who underwent abdominal surgery
resulting in pneumoperitoneum (arrow).
The pneumoperitoneum outlines the inferior border of the diaphram. This
facilitates identification
of the large subpulmonary plueral effusion.
The diagnosis of interlobar effusion can often be challenging, especially in the presence of incomplete pleural fissures. A CT may be required to make the diagnosis. Another challenge can be differentiating between a loculated effusion in the minor fissure and right middle lobe atelectasis. An effusion appears as an homogenous density with biconvex edges and preservation of the minor fissure, while atelectasis appears as an inhomogenous density with concave margins and obliteration of both the right heart border and minor fissure.
![]()
![]()