Emergency Ultrasound > RLQ Pain > Appendicitis
RLQ Pain - Appendicitis
![]()
Clinical
The differential diagnosis is often between gynecological and GI pathology. A RUQ US exam plus appendix or a pelvis plus appendix may have to be done depending on the clinical situation. CT is the preferred exam in the obese or elderly, or in patients who are in so much pain that a technically adequate ultrasound cannot be performed. The classic presentation is of a 10-30 year old person with right lower quadrant pain, nausea, vomiting, and leukocytosis. The presence of fever is evidence of perforation.
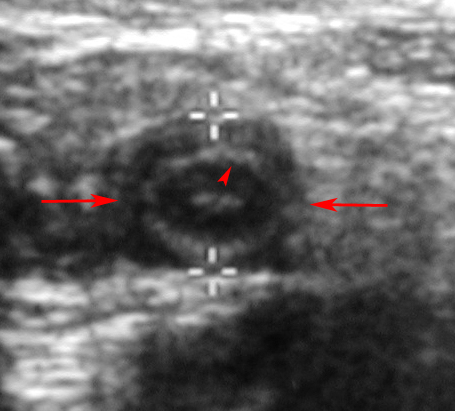
Transverse image reveals normal appendix (between red arrows and + cursors) and its echogenic submucosa (red arrowhead).
Exam
Use a linear probe (generally 5 MHz) and in transverse orientation press down the anterior flank. Use slow, graded compression. Compression should be strong enough that the anterior abdominal wall is pressed against the psoas muscle. If the patient is in too much pain, they may need sedation. If you cannot press like this, you must say it is a technically inadequate exam. When done correctly (with adequate compression), this is a specific and sensitive exam ( > 90%). Don't mistake the psoas for a abscess. If unsure, compare with the opposite side. If present, measure fecolith and diameter of appendix. Measure any loculated fluid collection.
The sensitivity of US decreases with perforation. With careful technique, a periappendicial abscess can be picked up with ultrasound. Therefore, thoroughly examine the RLQ (even the LLQ) for an inflammatory mass. If perforation is likely, consider CT instead of ultrasound.
Sonographic Diagnosis
Visualization of an aperistaltic tubular structure > 6 mm in diameter or visualization of an appendix with a fecolith confirms the diagnosis. Generally, the abnormal appendix is not at all subtle. The wall appears hypoechoic and may be strikingly so with impending perforation. A loculated fluid collection may represent abscess from a perforated appendix or other bowel source such as IBD, or GYN source such as TOA.
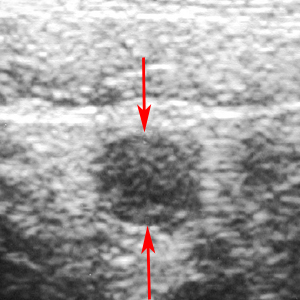
Transverse image reveals an 8-mm diameter, non-compressible appendix (between red arrows).

An obstructing appendicolith (red arrow, between + cursors) casts an acoustic shadow (S) and obstructs and dilates the appendix (A) resulting in acute appendicitis.
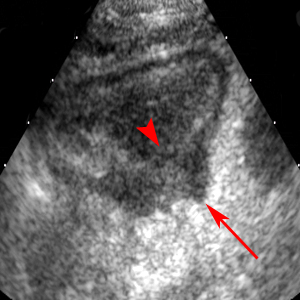
mage in the long axis of the appendix shows long segment loss of visualization of the submucosa (red arrowhead) and a focal perforation (red arrow).
![]()
![]()