Emergency Ultrasound > Flank Pain > Nephrolithiasis
Flank Pain - Nephrolithiasis
![]()
Clinical
Nephrolithiasis has its highest prevalence in men aged 20-40 years. Approximately 12% of men and 5% of women experience renal colic caused by stone disease at least once in their lifetimes. Most renal stone disease is idiopathic. Patients usually present with flank plain radiating to the genitals, nausea, vomiting, and constant motion. Ultrasound reliably demonstrates stones > 5mm size, but smaller stones, up to 40%, are commonly not detected. CT is commonly used for detection and is excellent.
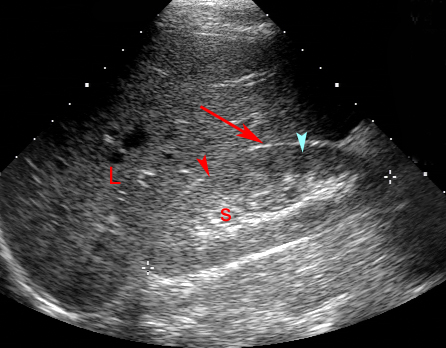
The renal cortex (red arrowhead) is equal in echogenicity to the liver parenchyma (L). The renal pyramids (blue arrowhead) are slightly hypoechoic compared to the renal cortex. The central renal sinus (s) is invested with echogenic fat. The red arrow indicates the location of Morrison's pouch.
Exam
Kidneys are usually best seen with the patient in the decubitus position. Document kidney size and the position and size of stones, cysts or masses. Confirm if cysts are simple (simple = round or oval, smooth walled, anechoic and increased through transmission). If cysts are not simple, they are indeterminate by US and may require further evaluation by CT.
Obtain multiple long and transverse images of each kidney including upper, mid and lower poles. Also get long axis of both kidneys showing comparison of renal echogenicity to adjacent liver or spleen. If hydronephrosis is seen, try to image ureter and assess level and cause of obstruction. Long and transverse images of the bladder, including ureteral tunnel views if indicated (r/o stone).
Measure kidney size in long, AP and transverse. Measure dominant cysts, masses or stones. Normal kidney size is 8-13 cm long. Normal echogenicity is iso or hypoechoic to normal liver.
Non-contrast spiral CT scan: consider using stone protocol CT for a symptomatic calculus instead of ultrasound.
Sonographic Findings:
1) Both radiopaque and radiolucent calculi produce highly echogenic foci with acoustic shadowing.
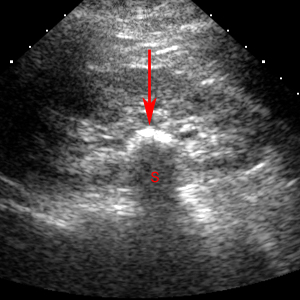
Solitary renal stone produces a bright echogenic focus (red arrow) in the renal sinus and casts an acoustic shadow (S).
2) Obstructing stones in the ureter are dectected by following the dilated ureter to the point of obstruction. Color Doppler can produce twinkling sign within or just distal to urinary tract calculi.
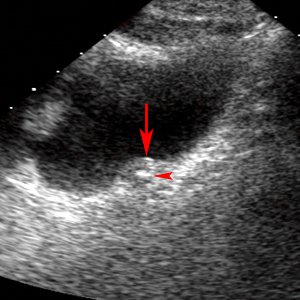
Longitudinal image of the bladder reveals a dilated uterovesical junction (red arrow) with a small impacted stone (red arrow head).
![]()
![]()