Emergency Ultrasound > Flank Pain > Hydronephrosis
Flank Pain - Hydronephrosis
![]()
Clinical
US demonstration of hydronephrosis is not, by itself, diagnostic of urinary obstruction. Hydronephrosis is an anatomic finding, not a functional one, and is caused by acute or chronic urinary obstruction, prostatic hypertrophy, strictures, vesicoureteral reflux (VUR), pregnancy, high urine output states, and congenital dilatation of the collecting system.
A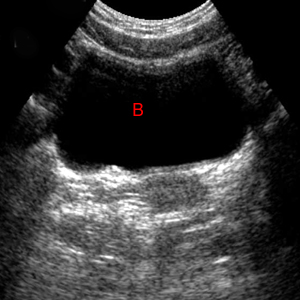 B
B
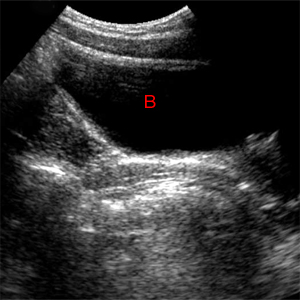
Bladder. A. Transverse. B. Longitudinal. Normal images of the bladder (B).
Exam
Obtain multiple long and transverse images of each kidney including upper, mid and lower poles. Get long axis of both kidneys showing comparison of renal echogenicity to adjacent liver or spleen. If hydronephrosis is seen, try to image ureter and assess level and cause of obstruction. Obtain long and transverse images of the bladder, including ureteral tunnel views if indicated (r/o stone)
A comprehensive renal exam must include the urinary bladder. If the bladder is empty, the collapsed bladder or bladder area must be documented. The distal ureters/ureteral tunnels should be imaged if stones are suspected.
Sonographic Findings:
1) Dilation of calyces, pelvis, and ureter. Calyces appear rounded and cystic and communicate with the renal pelvis.
2) Absence of ureteral jet on the affected side during several minutes of observation confirms complete obstruction.
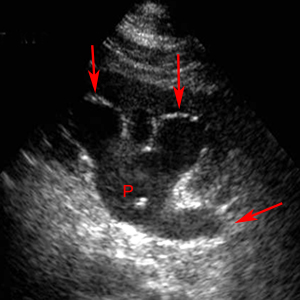
Hydronephrosis. Rounded calyces filled with urine (red arrows) connect to the fluid distended pelvis (P).
3) Intrarenal artery resistive index (RI) > 0.70 is highly suggestive of obstruction.
![]()
![]()