Emergency Ultrasound > RUQ Pain > Biliary Dilatation
RUQ Pain - Biliary Dilatation
![]()
Clinical
US is approximately 90% accurate in differentiating obstructive from non-obstructive jaundice by depicting the presence of biliary dilatation. Causes for biliary dilatation are impacted gallstone in CBD or at ampulla, benign stricture, pancreatic carcinoma , cholangitis, biliary surgery, and chronic pancreatitis.
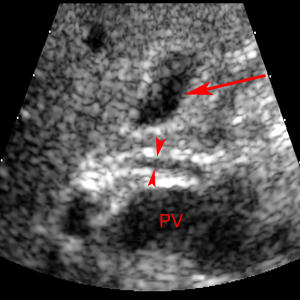
In the transverse image, the common bile duct (red arrowheads) is anterior to the portal vein (PV) and the gallbladder (red arrow) is also visualized.
Exam
Begin with the patient in the left posterior oblique position. Patient may also be placed in the supine position. Obtain longitudinal and transverse views of right and left lobe of liver and include longitudinal images of liver/diaphragm interface. Measure intrahepatic bile duct, common hepatic duct (CHD), and CBD as far distal as possible. Acquire longitudinal view of bile duct in pancreatic head and take measurement. Document patency in portal veins, hepatic veins, and hepatic artery.
Sonographic Findings:
1) Shotgun sign - intrahepatic biliary ducts (IHBD) become tortuous and their diameter exceeds 2 mm or exceeds 40% of the diameter of the adjacent PV. Color Doppler is used to confirm the absence of blood flow in the enlarged biliary tubes.
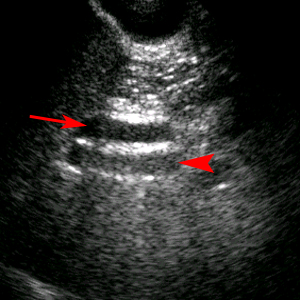
Shotgun Sign. Transverse image reveals dilated bile duct (red arrow) anterior to the portal vein (red arrowhead) resembling a double-barrel shotgun.
2) Confluence of enlarged intrahepatic biliary ducts (IHBD) create a stellate appearance of merging tubes.
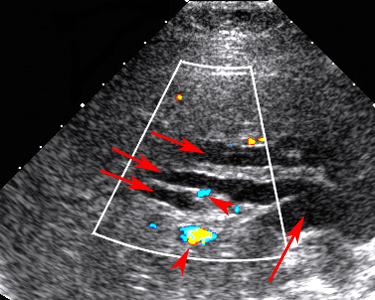
Dilated IHBD (red arrows) are seen as tortuous tubular structures in the liver. Color Doppler makes differentiation of bile ducts (red arrows) and blood vessels (red arrowheads) easy.
3) CBD is considered dilated in adults if its diameter > 7mm.
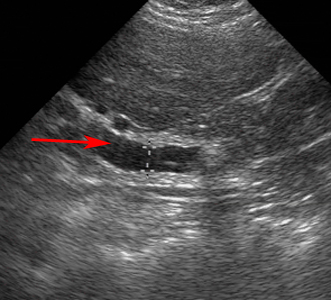
Dilated common bile duct (red arrow) measured at 9.7 mm.
![]()
![]()