PET/CT > Physics > Attenuation
Attenuation Correction
![]()
Attenuation is the loss of detection of true coincidence events because of their absorption in the body or due to their scattering out of the detector field of view. Attenuation problems are greater with PET imaging compared to traditional nuclear medicine SPECT imaging. Even though the photons are of greater energy than those used in SPECT imaging, in PET imaging two photons must escape the patient simultaneously to be detected as a true event and the mean photon path distance from emission to detection is greater with a PET camera than with a SPECT camera. The loss of true coincidence event detection due to attenuation in PET imaging can range between 50 to 95%, especially great in a larger person.
Loss of counts due to attenuation increases image noise, image artifacts, and image distortion. Without attenuation correction, significant artifacts which may occur on whole-body PET scans include: (1) prominent activity at body surface edges due to relative lack of attenuation at the surfaces compared to deeper structures, (2) distorted appearance of areas of intense activity (e.g. urinary bladder) due to variable degrees of attenuation in different directions of activity originating from these areas, and (3) diffuse, relatively increased activity in tissues of relatively low attenuation (e.g. lungs).Therefore, attenuation correction of data is necessary for accurate qualitative (i.e. visually normal, increased, or decreased) and quantitative (i.e. standardized uptake values or SUVs) measurements of FDG activity.
In PET/CT x-rays from a CT scan are used to construct an attenuation map of density differences throughout the body that can then be used to correct for the absorption of the photons emitted from FDG decay. Attenuation is much more likely in the center of the body and therefore non-attenuation-corrected images will show diffusely lower level activity deep in the body compared to the skin surface. The attenuation correction process essentially "adds counts back" into areas that are more attenuated due to their being deeper or being surrounded by relatively dense structures. Similarly, it essentially "subtracts counts" from areas that are attenuated much less than all other tissues (e.g. lungs and body surfaces). Both attenuation-corrected and non-attenuation-corrected data sets are provided for review and both should be examined by the interpreter. Reviewing both data sets sometimes allows confirmation of an abnormality or confirmation of the benignity of a process which might have been incorrectly assessed based on review of one set alone.
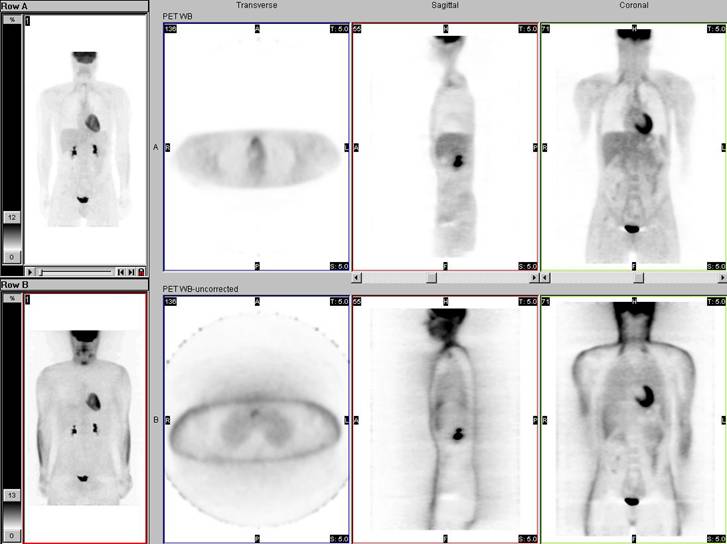
The top row displays attenuation-corrected PET data; the bottom row shows non-attenuation-corrected PET data.
Activity within tissue closely approximated to very high density material in the body may appear falsely low in intensity on attenuation-corrected data. For example, in correcting for attenuation by metallic density orthopedic hardware the computer may essentially "subtract" counts from the area immediately adjacent to the hardware which could at times include "subtraction" of true counts originating from an abnormality such as a lymph node. Close inspection of the CT data and non-attenuation-corrected PET data should permit accurate detection (or at least confirm suspicion) of the abnormal activity within the lymph node in that example.
Activity within tissue closely approximated to very high density material in the body may appear falsely high in intensity on attenuation-corrected data. For example, in correcting for attenuation by metallic density orthopedic hardware the computer may essentially "add" counts into tissues immediately adjacent to the hardware which could at times result in the false appearance of increased activity within tissue (e.g. a lymph node) closely approximated to the hardware. Close inspection of the CT data and the non-attenuation-corrected PET data should confirm that the apparent increase in activity within the lymph node in that example was artifactual, related to the attenuation correction process. However, artifacts of activity related to the attenuation correction process can result in equivocal findings even after close inspection of all of the data.
Some lesions located near the surface of the body, such as skin lesions, are more obvious on non-attenuation-corrected data because of the generalized "subtraction" of counts from the surface related to absence of attenuation there compared to deeper structures. On close review, uptake in these lesions will usually be visible on the attenuation-corrected data as well.
![]()
![]()